
Fibromyalgia
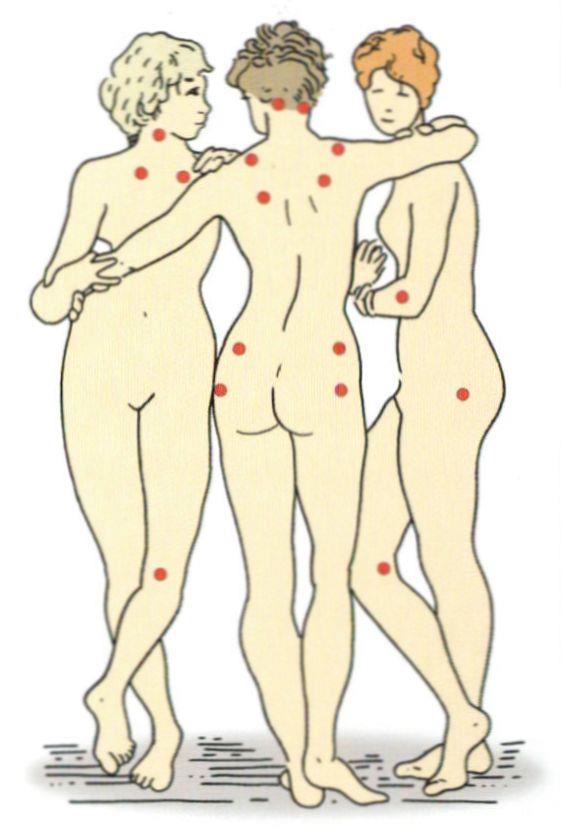
18 Triggerpunkte
Definition by MEDLINEPLUS:
Fibromyalgia is a disorder that causes muscle pain and fatigue. People with fibromyalgia have "tender points" on the body. Tender points are specific places on the neck, shoulders, back, hips, arms, and legs. These points hurt when pressure is put on them.
People with fibromyalgia may also have other symptoms, such as
Trouble sleeping
Morning stiffness
Headaches
Painful menstrual periods
Tingling or numbness in hands and feet
Problems with thinking and memory (sometimes called "fibro fog")
No one knows what causes fibromyalgia. Anyone can get it, but it is most common in middle-aged women. People with rheumatoid arthritis and other autoimmune diseases are particularly likely to develop fibromyalgia. There is no cure for fibromyalgia, but medicine can help you manage your symptoms. Getting enough sleep, exercising, and eating well may also help.
There exists a Widespread pain index (WPI) by which the following trigger points can be analysed and evaluated. Arm and Shoulder Tender Points
Chest Tender Points
Leg Tender Points
Head and Neck Tender Points
Back Tender Points
Buttock Tender Points
Control Points (Non-Tender Points are non-painful)
With the help of the Symptom severity scale it is possible to detect the tiredness, fatigue as well as cognitive symptoms and physical symptoms. Depending on the severity the patient can get 0- 3 points and 12 in total.
Scoring by ACR 2010:
Widespread Pain Index (WPI)
Part 1: Total the number of areas of tenderness or pain (out of 19 possible)
Symptom Score (SS)
Total the points from parts 2 and 3 (out of 12 possible)
Part 2: Total the number of points from the 3 questions (assign 0-3 points for each of the 3 questions)
Part 3: Assign 1 point for each of the 3 questions that are positive
Scoring by ACR 2010:
1. Widespread pain index (WPI)> = 7 and symptom severity scale (SS)> = 5
OR
WPI 3 - 6 and SS> 0 = 9.
2. The symptoms must persist in similar strength for at least 3 months.
3. The complaints are not caused by another illness.
There is also consensus regarding the following symptoms:
The core symptoms of FMS are, in addition to chronic pain in several body regions, sleep disorders or non-restorative sleep and tiredness or tiredness (physically and / or mentally).
To find a unique way how to evaluate and to treat a Fibromyalgia is one of the most interesting themes for me during the last few years. I think that there is nearly nothing which bothers a human more than completely reasonless pain. It would be much more bearable if our pain would have some kind of causing agent.
There were some scientists from Würzburg/ Germany who examined 25 patients and found a disorder of small nerve fibers which means that it is still possible that the Fibromyalgia has an organic or physical cause. Due to my opinion we can find out much more about this disease in the next years. 20 years ago no one would have thought that a simple bacterial infection by Heliobacter pylori is the causing agent for a gastric ulcer. For most of the patients who suffer from a Fibromyalgia the origin of the disease could be found in some kind of mislead neuronal process. Only the minority of cases can be explained with a physical or organic disorder.
Chronic pain can be compared to an earworm:
You have once heard a melody and cannot get rid of it anymore. You were just about to forget the melody when you hear it once again in some shop or in the TV. As more you concentrate on the melody as stronger and as louder the earworm gets. You can perform every possible examination from a MRT till an EEG but none of them will make you get rid of this earworm. The melody settled down in your neuronal network. No one will be able to find this earworm which is stuck in your head but anyways it is real, you will hear it!
The chronic pain follows the same principle. It gets triggered by an acute pain which then initiates some learning processes in the brain. The brain accomodates to the new situation to the pain which had a warning function in the beginning which means that the brain tries to focus on this possibly life threatening pain. This mechanism is a completely normal condition which appears in every human.
Now it is most important to treat the pain to prevent the formation of a pain memory. The acute pain needs some kind of psychosocial disposition or a disorder in the pain- processing system. The causes for this can be of genetic, hormonal, psychic, social, neuropsychologic or environmental origin. Recent perceptions of the epigenetic show that a behavior can be inherited 1- 2 generations. There were some studies in Atlanta (2014) about mice which inherit fear for 2 generations. Another example are post- war children who dream about war or feel fear in normal situations.
Disorders in the metabolism of the brain can have their origin in a learned or gentically inherited factor. That is why we must not differentiate between an organic or a psychic cause for the disease because the pain must not have a specific cause like an injury.
It is proven that patients who suffer from a Fibromyalgia do suffer from some kind of psychic disorder like depression or fear above the average. We cannot say if the psychic disorder is the cause for the pain or the pain is the cause for the Fibromyalgia but anyways we have to treat both.
According to my opinion we will differentiate the Fibromyalgia into a primary and a secondary in the upcoming years. This would be possible by the help of pain questionairy and a specific anamnesis to create the perfect therapy plan.
One of the most important steps to treat the disease is the realization of the disease as well as its origin because otherwise the disease will spread and occupy other parts of our every days life like sleeping, well- being or our social contacts. Therefore it is hard to treat the disease only with a drug therapy because it is essential to erase the pain memory.
So können mögliche Störungen im Hirnstoffwechsel Folge eines erlernten, weitergegebenen oder genetisch vorgegebenen Faktors sein. Letztendlich wird spätestens hier klar dass die strenge Unterscheidung zwischen organisch und psychisch sowohl haltlos als auch wenig zielführend ist. Unser Denken, dass eine Schmerz immer eine klare Ursache wie eine Verletzung als Ursache haben muß, war im Mittelalter revolutionär, ist heute aber überholt.
Bewiesen ist, dass bei Patienten mit Fibromyalgie überdurchschnittlich häufig psychische Störungen wie Depressivität und Ängstlichkeit vorkommen. Ob diese Patienten zuerst depressiv waren und darum Schmerzen entwickeln oder umgekehrt ist interessant, aber in keinster Weise zielführend für die Behandlung. Es gehört immer beides behandelt.
Es ist davon auszugehen dass in Zukunft die Fibromyalgie in eine primäre und eine sekundäre, eher psychosomatische Form differenziert wird. Das gelingt heute schon anhand der Schmerzfragebögen und der Anamnese. Danach orientiert sich dann auch die Behandlung.
Die Schmerzstörung hat die Tendenz sich auszuweiten und andere Bereiche des Lebens zu beeinträchtigen: Schlaf, Wohlbefinden, Verdauung, Leistungsfähigkeit, soziale Kontakte, Stimmung.....
Wichtig für die Behandlung ist das Verständnis der Grundlagen der Erkrankung. Die Erkrankung ist nur wenig durch Medikamente heilbar, sondern durch ein Verlernen des Schmerzgedächtnis.
Im Gegensatz zur landläufigen Meinung halte ich die Prognose für gut.
Due to the fact that a Fibromyalgia is caused by some kind of mislead learning process instead of any organic or physical disorder it is not possible to treat the disease with common therapies.
Strong therapy recommendation:
We try to create the perfect therapy plan with you which may include a multimordal therapy (combination of relaxing or cognitive therapy and stamina training), low intensity stamina training in combination with stretching exercises, Tai Chi or Yoga. It is hard to find the perfect medication but there are some drugs which have shown a positive effect
Middle therapy recommendation
1. Amitriptylin 10- 50 mg/d
Duloxetin 60 mg/ d
Off- label medicamentation (individual treatment plan): Dulxetin, Pregabalin or Seretonin inhibitors like Fluoxetin.
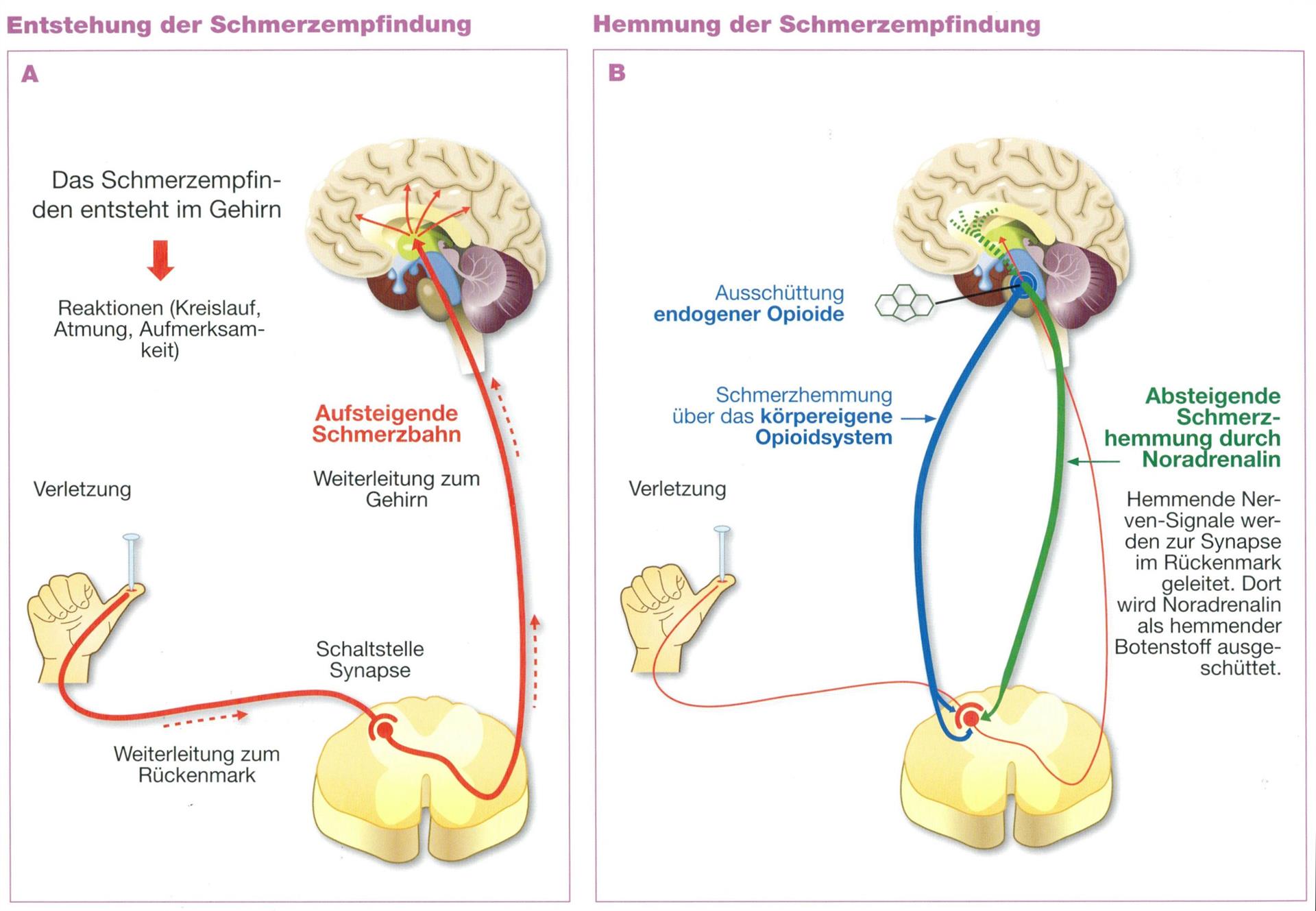
Die absteigende Schmerzhemmung (grüne Bahnen)
I made very good experiences with Amytriptilin but i want to explain the way the drug works otherwise you may ask yourself why your doctor prescribes you an antidepressant when reading the package insert. This can be explained with the way the brain handles pain because Amytriptilin decreases the threshold by enhancing the pain inhibition. The neurotransmitters Noradrenalin and Seretonin do not only inhibit pain but are also decreased in case of depression. To increase the pain inhibition the patient needs a dosage which is approximately 5- 10 times lower than the dosage to treat depressions.
Amitriptylin
Amytriptilin:
available commercially since 50 years
antidepressant
unselective inhibitor for Monoamin reabsorbtion from the synaptic cleft. Therefore an increase in Seretonin and Noradrenalin concentration
4- 10mg, in rare cases 25 mg/d
Dosage for Depressions: >50 mg /d
Perfect prophylaxis for tension headache or migraine
NOT applyable after cardiac infarction, EEG changes, Glaucoma
Possible side effects: fatigue, dryness of the mouth, increase in weight,
In the dosage which we prescribe side effects are very rare. The tiredness is a side effect which can be nice if it appears in the evening. That is why the drug gets ingested in the evening.
No recommendation
medications:
Anxiolytika (Valium), Cannabinoide, Flupirtin, Ketamin, Kortikosteroide, Lokalanästhetika, Milnacipran, Muskelrelaxantien, Natriumoxybat, Neurolpetika, Nichtsteroidale Antirheumatika (Ibuprofen, Diclofenac), starke Opioide, Serotoninrezeptor (5HT3) Antagonisten
Non-drug procedures
Chirotherapie, hyperbare Sauerstofftherapie, Lasertherapie, Magnetfeldtherapie, Massage, Nahrungsmittelergänzungsprodukte, TENS
Auszug aus den aktuellen Leitlinien:
Komplementäre Verfahren
|
Therapieverfahren |
Empfehlungsgrad 2008 |
Empfehlungsgrad 2012 |
|
Achtsamkeitsbasierte Stressreduktion als Monotherapie |
Keine Aussage |
Stark negative Empfehlung |
|
Akupunktur |
Stark negative Empfehlung |
Offene Empfehlung |
|
Atemtherapie |
Offene Empfehlung |
Keine Aussage |
|
Eliminationsdiät |
Offene Empfehlung |
Keine positive oder negative Empfehlung möglich |
|
Ergotherapie |
Offene Empfehlung |
Keine Aussage |
|
Fußzonenreflextherapie |
Offene Empfehlung |
Keine Aussage |
|
Homöopathie |
Offene Empfehlung |
Negative Empfehlung |
|
Meditative Bewegungstherapien |
Offene Empfehlung |
Starke Empfehlung |
|
Reiki |
Keine Aussage |
Negative Empfehlung |
|
Vegetarische Kost /Heilfasten |
Offene Empfehlung |
Keine positive oder negative Empfehlung möglich |
Medikamente
|
Therapieverfahren |
Empfehlungsgrad 2008 |
Empfehlungsgrad 2012 |
|
Amitriptylin |
Starke Empfehlung |
Empfehlung |
|
Anxiolytika |
Negative Empfehlung |
Stark negative Empfehlung |
|
Cannabinoide |
Nicht berücksichtigt |
Negative Empfehlung |
|
Dopaminagonisten |
Offene Empfehlung |
Stark negative Empfehlung |
|
Duloxetin |
Empfehlung |
Empfehlung bei komorbider depressiver oder generalisierter Angststörung |
|
Flupirtin |
Keine Aussage |
Negative Empfehlung |
|
Hormone (Calcitonin, Testosterone, Östrogene, Glukosteroide, Schilddrüsenhormone, Wachstumshormon) |
Negative Empfehlung |
Stark negative Empfehlung |
|
Hypnotika |
Negative Empfehlung |
Stark negative Empfehlung |
|
Ketamin |
Negative Empfehlung |
Stark negative Empfehlung |
|
Lokalanästhetika |
Negative Empfehlung |
Stark negative Empfehlung |
|
Milnacipran |
Keine Aussage |
Stark negative Empfehlung |
|
Monoaminooxidasehemmer |
Offene negative Empfehlung |
Negative Empfehlung |
|
Natriumoxybat |
Negative Empfehlung |
Stark negative Empfehlung |
|
Neuroleptika |
Negative Empfehlung |
Stark negative Empfehlung |
|
Nicht-steroidale Antirheumatika |
Negative Empfehlung |
Stark negative Empfehlung |
|
Metamizol |
Negative Empfehlung |
Keine positive oder negative Empfehlung möglich |
|
Muskelrelaxantien |
Offene negative Empfehlung |
Negative Empfehlung |
|
Opioide schwach (Tramadol) |
Offene Empfehlung |
Keine positive oder negative Empfehlung möglich |
|
Opioide stark |
Offene negative Empfehlung |
Stark negative Empfehlung |
|
Paracetamol |
Negative Empfehlung |
Keine positive oder negative Empfehlung möglich |
|
Pregabalin |
Offene Empfehlung |
Offene Empfehlung (offlabel-use) |
|
Serotoninwiederaufnahmehemmer (Fluoxetin, Paroxetin) |
Empfehlung |
Offene Empfehlung bei komorbider depressiver Störung |
|
Serotoninrezeptoragonisten (Topisetron) |
Offene Empfehlung |
Stark negative Empfehlung |
|
Virostatika |
Negative Empfehlung |
Stark negative Empfehlung |
Physikalische Verfahren und Physiotherapie
|
Therapieverfahren |
Empfehlungsgrad 2008 |
Empfehlungsgrad 2012 |
|
Chirotherapie |
Offen |
Negative Empfehlung |
|
Funktionstraining |
Offen |
Starke Empfehlung |
|
Krafttraining |
Nicht berücksichtigt |
Starke Empfehlung |
|
Ganzkörperwärme mit wassergefilterter milder Infrarot-A-Strahlung |
Empfehlung |
Keine positive oder negative Empfehlung möglich |
|
Ganzkörperkälte |
Offen |
Negative Empfehlung |
|
Krankengymnastik |
Offen |
Keine positive oder negative Empfehlung möglich |
|
Laser |
Offen |
Negative Empfehlung |
|
Lymphdrainage |
Offen |
Keine positive oder negative Empfehlung möglich |
|
Magnetfeld |
Offen |
Negative Empfehlung |
|
Massage |
Negativ |
Stark negativ |
|
Osteopathie |
Offen |
Keine positive oder negative Empfehlung möglich
|
|
Physiotherapie |
Offen |
Keine positive oder negative Empfehlung möglich |
|
Transkranielle Magnetstimulation |
Offen |
Negative Empfehlung |
|
Ultraschall/Reizstrom |
Offen |
Keine positive oder negative Empfehlung möglich |
Psychotherapie und Patientenkommunikation
|
Therapieverfahren |
Empfehlungsgrad 2008 |
Empfehlungsgrad 2012 |
|
Biofeedback |
Offen |
Offene Empfehlung |
|
Kognitive Verhaltenstherapien |
Offen |
Offene Empfehlung |
|
Patientenschulung als Monotherapie |
Nicht berücksichtigt |
Offene Empfehlung |
|
Therapeutisches Schreiben |
Empfehlung |
Negative Empfehlung |
Farbcodes:
Geänderte Datenlage (neue RCTs ab 2007)
Neue Kriterien für Auf- und Abstufung des Empfehlungsgrades von Therapien
Sowohl neue Datenlage als auch neue Kriterien für Auf- und Abstufung des
Empfehlungsgrades von Therapien